UOJM AHEAD OF PRINT
REVIEW
Asthma Prevalence in Canadian Indigenous Populations: A Systematic Review
2 Department of Biomedical and Molecular Sciences, Queen’s University, Kingston, ON, Canada
3 Schulich School of Medicine & Dentistry, Western University, London, ON, Canada
University of Ottawa Journal of Medicine, Ahead of Print, March 2026,
https://doi.org/10.18192/UOJM.V16i1.7465
Keywords: Asthma prevalence, Asthma risk factors, Respiratory disease, Canadian Indigenous, Canadian aboriginal.
Abstract
Asthma is a common respiratory disorder that disproportionately affects Indigenous Canadians, contributing to increased morbidity and healthcare disparities. Despite advances in understanding asthma pathophysiology, Indigenous populations experience a higher prevalence of asthma and poorer disease control due to social determinants of health. Limited research has explored the specific mechanisms through which these determinants affect asthma etiology and disease management within Indigenous communities. This review synthesizes existing evidence on asthma prevalence among Indigenous Canadians, examining the impact of socioeconomic status, geographic location, cultural barriers, and healthcare access. By identifying patterns in how social determinants contribute to asthma development and management, this review aims to inform strategies for improving respiratory health outcomes within Indigenous communities. A systematic search was conducted in PubMed, Medline OVID, and EMBASE using MeSH and keyword searches. Studies focusing on Canadian Indigenous populations and asthma epidemiology were included, while non-relevant and non-peer-reviewed articles were excluded. A total of 12 studies were analyzed, comprising cross-sectional surveys, cohort studies, and a randomized controlled trial. Findings indicate that asthma prevalence varies by sex, age, and with risk factors including overcrowded housing, low socioeconomic status, and limited healthcare access. Cultural barriers, such as the lack of Indigenous-centered asthma education, further hinder disease management. Addressing asthma disparities among Indigenous Canadians requires a multifaceted approach, including policy reforms, community-driven interventions, and the integration of culturally competent care. Incorporating Indigenous perspectives into national asthma frameworks can improve disease outcomes and respiratory health equity.
Résumé
L’asthme est une affection respiratoire courante qui affecte de manière disproportionnée les Autochtones du Canada, contribuant ainsi à une morbidité accrue et à des inégalités en matière de soins de santé. Malgré les progrès réalisés dans la compréhension de la physiopathologie de l’asthme, les populations autochtones présentent une prévalence plus élevée et un moins bon contrôle de la maladie en raison des déterminants sociaux de la santé. Toutefois, peu de recherches ont exploré les mécanismes spécifiques par lesquels ces déterminants influencent l’étiologie de l’asthme et la prise en charge de la maladie au sein des communautés autochtones. Cette revue synthétise les données existantes sur la prévalence de l’asthme chez les Autochtones canadiens, en examinant l’impact du statut socio-économique, de la situation géographique, des barrières culturelles et de l’accès aux soins de santé. En identifiant les schémas selon lesquels les déterminants sociaux contribuent au développement et à la prise en charge de l’asthme, cette revue vise à informer les stratégies pour améliorer les indicateurs de santé respiratoire au sein des communautés autochtones. Une recherche systématique a été menée dans PubMed, Medline OVID et EMBASE en utilisant MeSH et par mots-clés. Les études portant sur les populations autochtones canadiennes et l’épidémiologie de l’asthme ont été incluses, tandis que les articles non pertinents et non évalués par des pairs ont été exclus. Au total, 12 études ont été analysées, comprenant des enquêtes transversales, des études de cohorte et un essai contrôlé randomisé. Les résultats indiquent que la prévalence de l'asthme varie selon le sexe, l'âge et certains facteurs de risque, comme le surpeuplement des logements, un faible statut socio-économique et un accès limité aux soins de santé. Les barrières culturelles, telles que le manque de formation sur l’asthme axée sur les populations autochtones, entravent davantage la prise en charge de la maladie. Pour réduire les inégalités face à l’asthme chez les Autochtones du Canada, il faut adopter une approche multidimensionnelle, comprenant des réformes politiques, des interventions communautaires et l’intégration de soins adaptées à la culture. L’intégration des perspectives autochtones dans les cadres nationaux de lutte contre l’asthme peut améliorer les résultats de la maladie et l’équité en matière de santé respiratoire.
Introduction
Asthma is a major non-communicable disease of the respiratory system and has a significant impact on quality of life.1 Approximately 11% of Canadians are affected by asthma, a figure that is expected to increase as new immigrants continue to arrive in the country each year.2,3 Despite advances in understanding the pathology underlying asthma, and a steady decrease in incidence over the past 20 years, asthma continues to be a major contributor of respiratory morbidity in Canada.2,4
In comparing the prevalence of asthma between different populations in Canada, Indigenous communities provide a critical example of how the social determinants of health can influence both the incidence and the morbidity of a disease. Before European settlement, Indigenous peoples lived in self-governing communities and emphasized good health practices through active lifestyles and balanced, nutritious diets.5 However, the impacts of disease, land dispossession, and the forced separation of children from their families through the residential school system significantly disrupted traditional ways of life.6 Present-day Indigenous communities continue to face the enduring effects of colonialism as well as geographic separation from other communities in Canada.5 In the context of respiratory disease, these historical and socio-economic factors are reflected in the elevated prevalence of asthma, lower health literacy, and higher rates of emergency room visits due to poorly managed asthma symptoms.7-9 Furthermore, while the National Lung Health Framework (NLHF) acknowledges that Indigenous peoples are at higher risk for asthma, it lacks specific guidelines for asthma care tailored to these communities.10
Current evidence suggests that asthma is a multifactorial disorder, with a phenotype that is influenced by the intersection of genetic susceptibility, environmental exposure and social determinants.1 Although social determinants contribute to the higher burden of asthma among Indigenous Canadians, there is a paucity of literature exploring exactly how these determinants contribute to the etiology of asthma, and how healthcare strategies can address these determinants in treatment planning or prevention. This review aims to synthesize existing evidence on the influence of social determinants on the development and management of asthma within Indigenous communities in Canada. By elucidating key patterns, it seeks to generate insights that can inform culturally grounded strategies for improving asthma care. Ultimately, these findings may help advance health equity and enhance asthma control among Indigenous populations.
Methods
Article Collection
All articles were collected from the electronic databases PubMed, Medline OVID and EMBASE. The search involved a combination of MeSH (Medical Subject Headings), keywords, and title and abstract searches, utilizing a mix of general terms related to our topic, health concepts, health conditions, Indigenous terms, cultural and historical factors, and socioeconomic terms that are outlined in Table 1.
Table 1. MeSH Terms and Keywords Used in the Literature Search
| Category | MeSH Terms & Keywords |
|---|---|
| General Terms | Pathology, Pathological, Disease Trend, Epidemiology, Epidemiological, Health Disparities, Health Inequities, Health Inequity, Health Inequalities, Health Inequality |
| Health Concepts | Environmental Health, Social Determinants of Health, Risk factors, Morbidity trends, Mortality trends, Health trends, Disease monitoring, Health indicators |
| Health Conditions | Cancer, Cardiovascular Disease, Infectious Disease, Chronic Disease, Mental Health, Substance Use, Addiction, Respiratory Disease, Diabetes Mellitus, Obesity, Trauma and Injury, Occupational Disease, Environmental Exposure, Neoplasms, Heart diseases, Communicable diseases, Wounds and injuries |
| Indigenous Populations | Indigenous, Aboriginal, Native people of Canada, Native Canadian communities, First Nations, Métis, Inuit |
| Cultural and Historical Factors | Traditional medicine, Colonialism, Acculturation |
| Socioeconomic Factors | Socioeconomic Factors, Health Services Accessibility, Population Surveillance, Canada, Geographic Disparities, Regional Variation, Healthcare Utilization, Urbanization, Remote Communities, Canadian Health Trend, Poverty, Low income, Low SES, Low socioeconomic status, Population dynamics |
Article Selection
The inclusion criteria for this study encompassed articles that 1) were published in English; 2) focused on Canadian Indigenous populations; and 3) discussed asthma epidemiology. Articles were excluded if they: 1) focused on non-Canadian populations; 2) focused on pathologies unrelated to asthma; and 3) were not full articles (including abstracts and posters) or had been retracted. Two authors independently screened titles and abstracts against the inclusion criteria. Potentially eligible full-text articles were retrieved and assessed in detail by the same authors. Discrepancies were resolved through discussion or adjudication by a third author. The study selection process is illustrated in the PRISMA flow diagram (Figure 1).
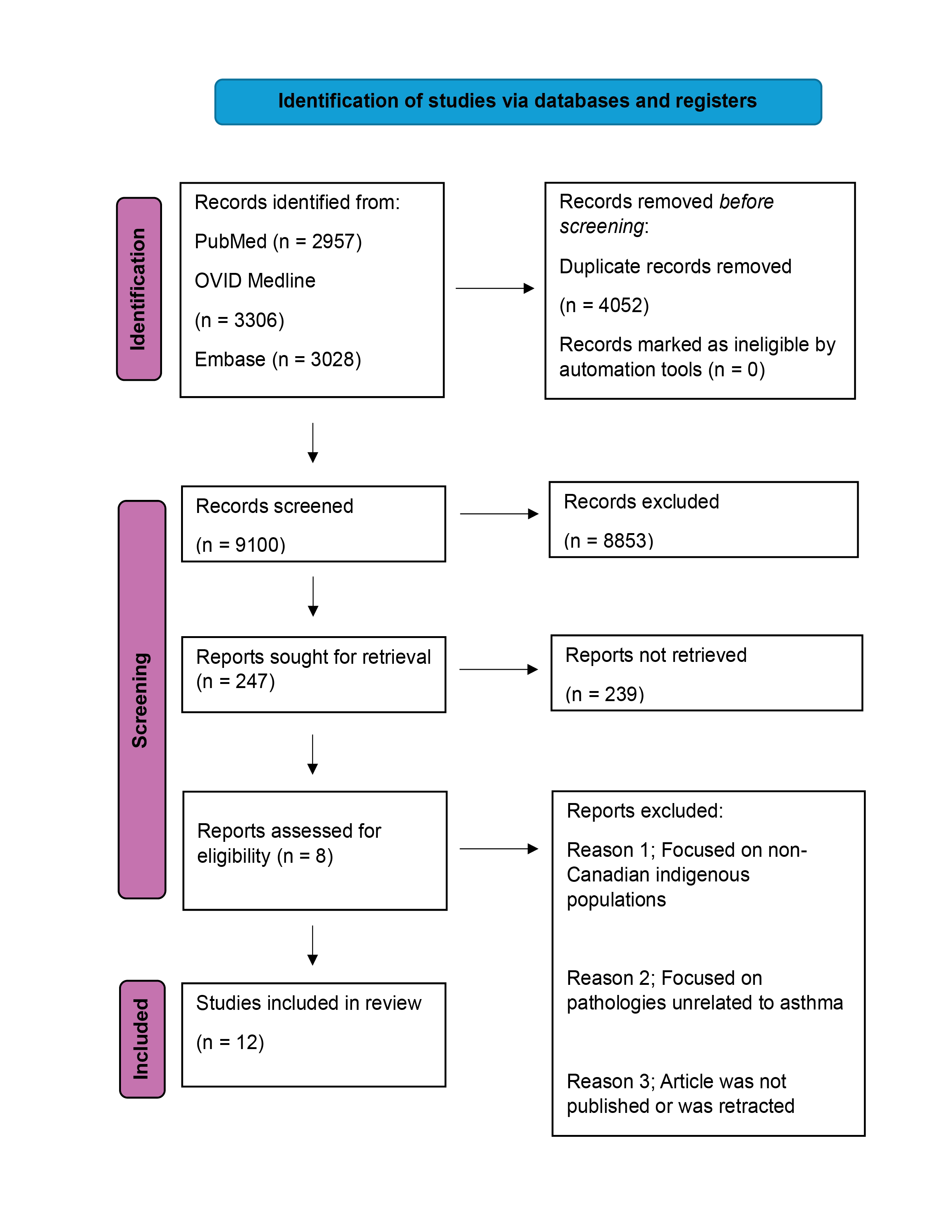
Figure 1. PRISMA flowchart for article selection.
Data Extraction
Data were extracted independently and in duplicate using a standardized data extraction form. The following data were collected: author(s), year of publication, study design, sample size, population characteristics (including specific Indigenous group, age, sex), geographic region, asthma definition, prevalence or incidence rates, and reported risk factors or determinants. Any disagreements were resolved through discussion. All relevant data that fit the aim of the study was included in Table 2.Table 2. Summary of asthma epidemiology in various Canadian Indigenous populations (12 articles)
| Author | Modality | Indigenous Population Studied | Outcomes | Drawbacks | |
|---|---|---|---|---|---|
| Fenton et al., 201210 | Telephone surveys, Focus groups | First Nations (n=15), Inuit (n=15) | -Identified asthma risk factors and barriers to care. -Highlighted lack of community resources, education, and healthcare services for asthma. -Explored methods for culturally appropriate care integration. |
-Telephone surveys may introduce response bias. -Low sample size. -Results cannot be generalized to all Indigenous populations |
|
| Sin et al., 20027 | Electronic Database | Aboriginals | -2.1x more emergency visits and 1.6x more office visits for asthma than non-Aboriginals. -55% less likely to see a specialist. -66% less likely to undergo spirometry testing. -Higher asthma rates than low-income non-Aboriginals. -Multiple factors contribute to increased respiratory burden. |
-Asthma prevalence was solely determined by physician diagnosis and did not account for diagnostic error. -The study did not consider Aboriginal patients treated by nurse practitioners. |
|
| Afzal, 20029 | Interviewer-administered questionnaires, Clinical testing | First Nations (n=956) | -Atopic asthma: 11.4% in First Nations. -Nonatopic asthma: 5% in First Nations. -Higher nonatopic asthma in First Nations women 40+ vs. men. -Depression increases atopic asthma risk 2.9x. -Nonatopic asthma causes: home dampness, alcohol use, co-morbidities. -Financial strain linked to nonatopic asthma in women, not men. |
-Social desirability bias may have affected questionnaire responses. -Limited research on asthma by sex made comparisons difficult. -Low sample size for older age groups. -Self-reporting may have led to measurement errors. -Excluding participants with anaphylaxis/eczema may have underestimated asthma prevalence. -Only non-food allergens were tested, possibly underestimating atopy prevalence. -Family history of asthma was not measured. -Combining two First Nations communities may have masked differences. -Response rates varied (53.9% vs. 89.9%), creating selection bias. |
|
| Riva et al., 202018 | Prospective (before-after) | Inuit (Nunavik/Nunavut) | -Decreased asthma symptoms and psychological distress after housing relocation | -Self-reported symptoms | |
| Koleade et al., 201814 | Survey (n=28,410) | Aboriginal | -ACO prevalence: 1.65% in males, 3.53% in females. -Risk factors: age, Quebec residence, poor housing, low income. -Female-specific risks: divorce/widowhood, smoking, diabetes, 40h+ work weeks. |
-Possible response and social desirability bias. -No spirometry confirmation, risk of misclassification. -Workplace exposures not considered. |
|
| Karunanayake et al., 202011 | Survey (n=24,803) | Aboriginal | -Lifetime asthma in Aboriginal adolescents: 16%. -Prevalence: 16.8% in boys, 15.3% in girls. -Risk factors: age, income, obesity, smoking, children in household, bronchitis history, urban living, education, location. -Female sex protective against lifetime asthma diagnosis. -Higher asthma diagnosis in Aboriginal adolescents vs. general population. -Obesity protective against asthma diagnosis. |
-Possible response and social desirability bias. -No explanation for obesity’s protective effect. -Missing factors (e.g., allergy, family history) may underestimate prevalence. -Temporal variations not considered. |
|
| Koleade et al., 202015 | Survey (n=28,410) | Aboriginal | -ACO prevalence in Aboriginal population: 2.7%. -Risk factors: age, income, marital status, urban living, Ontario/Quebec residence, poor housing, small dwelling, 80+ hour work weeks, smoking, diabetes. -Women 2x more likely to have ACO than men. |
-Survey/self-reports may have response or social desirability bias. -Single time-point data collection risks self-reporting bias/misclassification. -Self-reported asthma diagnosis lacks clinical accuracy. |
|
| Senthilselvan et al., 201512 | Survey (n=6657) | First Nations | -Ever-asthma prevalence: 14.6% (12.6% in 0–4 yrs, 15.6% in 5–11 yrs). -Higher in boys (16.1%) than girls (13.2%). -Risk factors: crowded homes, inactivity, low income, smoking, breastfeeding, high daycare/school attendance, isolated communities. -Stronger allergy-asthma link in low-birth-weight children. -Stronger chronic ear infection-asthma link in girls. -Similar ever-asthma prevalence among First Nations, Aboriginal, and non-Aboriginal children. |
-Survey may have resulted in response bias or social desirability bias. -Temporal variations between exposure and outcome were not accounted for. |
|
| Chang et al., 201213 | Survey, Questionnaires, Personal and Telephone Interviews (n=48,921) | Aboriginal | -Asthma prevalence: 14.3% (children), 14% (adults). -Child risk factors: male sex, allergy, low birth weight, obesity, poor housing, urban residence. -Adult risk factors: age, female sex, living alone, low income, urban residence. -Lower asthma prevalence in Aboriginal children, higher in Aboriginal adults vs. Canadian population. -Non-urban living is a protective factor for ever-asthma. |
-Temporal variations between exposure and outcome not considered. -Data quality/validity may vary by collection method (personal vs. telephone interviews). |
|
| Gao et al., 200816 | Surveys, personal interviews, telephone interviews and questionnaires (n=2404) | Aboriginal | -Asthma lower in Aboriginal (5.7%) vs. non-Aboriginal children (10%). -Infants/toddlers (30%) had more asthma-like symptoms than preschool (21.5%) & school-aged (11.5%). -Risk factors: allergy, maternal smoking. -Higher asthma prevalence in female Aboriginal children than males. |
-Possible response or social desirability bias. -Sample too small for <4 years asthma prevalence. -Survey lacked asthma focus, possibly underestimating rates. |
|
| Kovesi et.al., 20098 | Double-blind Randomized Control Trial (n=51) | Inuit (Nunavut) | -Significant reduction in wheeze and rhinitis -Improved indoor air quality |
-Small sample size -Unclear impact on health center visits |
|
| Crighton et al., 201017 | Survey (n=60,500) | Indigenous groups in Canada | -12% of Aboriginal children had an asthma diagnosis. -Higher prevalence in boys and the oldest age group. -Highest asthma rates in urban areas, off-reserve, and Ontario. -Key risk factors: Low income, older/damaged homes, single-parent households, low parental education, living in Quebec or Ontario. -Most common in the 0-4 age group. -Higher prevalence in Aboriginal women than men. -Geographic location impact: Lower diagnosis rates in northern territories, on-reserve, and rural areas. -Asthma medication use: Lowest in Quebec (41.7%), highest in British Columbia (68.9%). -Increased medication use linked to low education, poor housing, middle-income, female sex, old age, and Inuit identity. -Geographic location & Aboriginal identity significantly influenced medication use. |
-Potential biases: Response bias and social desirability bias. -Cross-sectional design limits ability to determine causation. -Limited generalizability due to missing data and excluded communities. -Confidentiality restrictions prevented identification of some population groups. -Self-reports may include false memories or misdiagnoses. -Key exclusions: Adult asthma medication use and second-hand smoke exposure. |
|
Risk of Bias Assessment
The methodological quality of the included studies was evaluated using the Newcastle-Ottawa Scale (NOS) for observational studies. The NOS evaluates studies based on selection of participants, comparability of study groups, and outcome/exposure assessment. NOS scores were determined based on the presence of potential sources of bias identified in each study’s methodology, with a maximum possible score of 9. Risk of bias was categorized as low (scores of 7–9), moderate (scores of 5–6), or high (scores below 5). Each study was assessed independently by two authors, and discrepancies were resolved by consensus. A full breakdown of study-level NOS scores and associated risk categories is provided in Table 3.Table 3. Risk of Bias Summary Table (12 articles)
| Author | Modality | NOS Score | Risk of Bias |
|---|---|---|---|
| Fenton et al., 201210 | Telephone surveys, Focus groups | 8 | Low |
| Sin et al., 20027 | Electronic Database | 9 | Low |
| Afzal, 20029 | Interviewer-administered questionnaires, Clinical testing | 7 | Low |
| Riva et al., 202018 | Prospective (before-after) | 7 | Low |
| Koleade et al., 201814 | Survey (n=28,410) | 7 | Low |
| Karunanayake et al., 202011 | Survey (n=24,803) | 8 | Low |
| Koleade et al., 202015 | Survey (n=28,410) | 6 | Moderate |
| Senthilselvan et al., 201512 | Survey (n=6657) | 7 | Low |
| Chang et al., 201213 | Survey, Questionnaires, Personal and Telephone Interviews (n=48,921) | 7 | Low |
| Gao et al., 200816 | Surveys, personal interviews, telephone interviews and questionnaires (n=2404) | 8 | Low |
| Kovesi, 20098 | Randomized Control Trial (n=51) | 7 | Low |
| Crighton et al., 201017 | Survey (n=60,500) | 4 | High |
Results
The initial search criteria yielded 9291 articles (PubMed: 2957, OVID Medline: 3306, EMBASE: 3028), of which 4052 duplicates and 7 retracted papers were removed leaving 5232 papers for further screening. The title screening narrowed the selection to 247 articles. Subsequent abstract review reduced this number to 8, and full-text evaluation ultimately identified 4 papers for inclusion. Finally, a manual search on Google yielded 8 additional articles for a total of 12 articles that fit the inclusion criteria. Articles were excluded based on a predetermined exclusion criterion. A summary of the findings from each article is detailed in Table 2.
The study design of the 12 articles analyzed comprised one mixed-method design, one retrospective cohort study, one randomized controlled trial, one prospective study and eight cross-sectional surveys. The majority of the data analyzed in the eight survey designs was obtained from various iterations of the Aboriginal Peoples Survey (APS), a national survey of Canadian First Nations, Metis and Inuit populations. The APS provided valuable insights into asthma prevalence by sex, age, Indigenous population and geographical location while shedding light on risk factors for asthma. While most of the studies outlined similar risk factors for asthma, there was no clear consensus as to which sex and Indigenous population was disproportionately affected by asthma.
Quality Assessment of Included Studies
The methodological quality of the 12 included studies was generally high, as assessed using the Newcastle–Ottawa Scale (NOS) (Table 3). Eleven studies achieved scores ranging from 7 to 9, indicating a low risk of bias, while one study scored 6 and was rated as moderate risk.7-16,18 Only one study, Crighton et al. (2010), received a high-risk rating (score = 4) due to limitations in sampling representativeness and missing data.17 The consistent use of large national survey datasets (e.g., APS) and robust recruitment strategies strengthened the validity of most studies.9-13,17 However, reliance on self-reported outcomes, cross-sectional designs, and the absence of clinical confirmation of asthma diagnoses introduced potential response and recall biases.9-13,16,17 Overall, the predominance of low-risk studies supports the reliability of the synthesized evidence, though the interpretability of findings is somewhat constrained by the few studies with methodological limitations.
Asthma Risk Factors Identified Across the Included Studies
Across the 12 studies included in this review, several recurring risk factors for asthma were identified among Canadian Indigenous populations. Environmental and lifestyle-related factors such as crowded housing, poor ventilation, household dampness, smoking exposure, and urban residence were frequently associated with asthma prevalence and symptom severity.7,11-13,16,17 Socioeconomic conditions, including low income, limited education, and unemployment, were also consistently linked to elevated asthma risk.9,11,13,15,17 Multiple studies highlighted biological and clinical factors such as obesity, chronic bronchitis history, allergies, low birth weight, and comorbidities including diabetes and chronic obstructive pulmonary disease (COPD), which were found to influence asthma development and exacerbation.9,11-15,16,17 Sex-based differences were observed across several studies: Indigenous women exhibited higher rates of asthma and asthma–COPD overlap (ACO) than men, whereas higher asthma prevalence among boys was reported in some child and adolescent cohorts.9,11,12,14-17 In addition, smoking, long working hours, and urban living were consistently identified as risk enhancers across both sexes.14,15,17 One of the included randomized controlled trial studies demonstrated that improving indoor air quality through ventilation interventions significantly reduced wheeze and rhinitis symptoms in Inuit children, underscoring the impact of environmental modification.8 Overall, these findings suggest that asthma in Indigenous populations is influenced by an intersection of environmental exposures, lifestyle behaviors, and socioeconomic disadvantage.
Social Determinants Influencing Asthma Epidemiology
The included studies also revealed that asthma prevalence and management among Indigenous Canadians are profoundly shaped by social determinants of health. Socioeconomic status (SES) was repeatedly cited as a major determinant, with low income, unemployment, and reduced access to education associated with higher asthma rates and poorer outcomes.9,11,13,15,17 The quality of housing emerged as a critical factor, with overcrowding, household dampness, and poor ventilation consistently linked to greater respiratory morbidity.7,12,13,17,18 Geographic isolation and remoteness further compounded these disparities by limiting access to healthcare resources, diagnostic services, and medication use.10,17,18 Cultural and systemic barriers, including the lack of Indigenous-centered asthma education materials and limited culturally competent healthcare services, were identified as additional obstacles to effective asthma management.10 Together, these social determinants interact with environmental and biological factors to perpetuate asthma disparities across diverse Indigenous populations in Canada.
Discussion
Strengths and Limitations of the Selected Articles
A notable strength of utilizing the APS for data collection was the large sample size (n>10,000) consisting of various Canadian Indigenous populations. However, the cross-sectional nature of the survey limits its ability to capture temporal variations in asthma prevalence.11-13 In addition, the possibility of response bias and social desirability bias is an inherent limitation of the survey design.
Of the assessed studies, most received a low risk of bias rating, with NOS scores ranging from 7 to 9, with the exception of one study. A commonality across almost every study was the identification of risk factors for asthma.7-17 Kovesi et al. (2009) employed a double-blind randomized controlled trial design, strengthening the internal validity of their findings, and demonstrated a measurable reduction in asthma-related symptoms following an environmental intervention.8 Riva et al. (2020) used a large, community-based, prospective design to assess real-world housing improvements and their impact on self-reported asthma symptoms.18 However, both studies have limitations. Kovesi et al. (2009) was limited by a small sample size and short follow-up period, which may restrict the generalizability of findings.8 Riva et al. (2020) relied entirely on self-reported outcomes without clinical validation, and the study population was limited to Inuit adults in social housing, which may not reflect the broader Indigenous population.18 Despite these limitations, both studies were assessed to be at low risk of bias and offer important context-specific insights for public health interventions.
Among the original research studies, Fenton et al. (2012) provided a significant contribution by identifying barriers to healthcare access for Indigenous populations and proposing culturally appropriate solutions.10 On a similar note, Sin et al. (2002), showed that Aboriginal populations were less likely to utilize testing services for asthma.7 However, a common limitation to the studies conducted by Fenton et al. (2012), and Sin et al. (2002), was the exclusion of relevant participants through low sample size.7-10
A significant strength of the studies conducted by Koleade et al. (2018, 2020), was the inclusion of patients with ACO and the identification of female-specific risk factors for asthma.14,15 However, ACO cases were self-reported and not clinically confirmed, leading to the possibility of disease misclassification and overestimates of ACO prevalence.14
Among the 12 included studies, Crighton et al. (2010), was the only one to draw connections between asthma medication use rate and asthma prevalence, offering a valuable perspective on treatment patterns.17 However, the same study was limited by the fact that the survey excluded some Indigenous populations, limiting generalizability.17
Overall, despite methodological differences, the reviewed studies largely converged on common asthma risk factors and prevalence trends across diverse Indigenous populations in Canada.7-18 This facilitated an examination of asthma prevalence in relation to age, sex, and population type.
Socioeconomic Status and Geographic Location
To understand asthma in the context of Indigenous health, it is essential to examine the broader systemic factors that contribute to healthcare disparities. One major issue is the lack of access to adequate housing, overcrowding, and an isolated community.12 Due to ongoing infrastructure crises on reserves, lack of available housing units and lack of construction materials, many Aboriginals resort to overcrowding, often exceeding the recommended occupancy limits.19 Due to the increased humidity caused by multiple people living together, mold growth and poor ventilation can lead to asthmatic symptoms and irritation of the respiratory tract epithelium.20 The situation is further compounded by inadequate maintenance measures to prevent mold accumulation and the absence of proper ventilation systems in homes.19,21
At the core of these housing challenges is the issue of low SES, which has been consistently linked to health disparities in Indigenous communities, including higher asthma prevalence.22 Notably, this disparity persists even among Indigenous populations living off-reserve.22 The most striking example of income disparity is seen in First Nations people, have a median annual income of only $14,000 as of 2005, far below Canada’s official 2023 poverty threshold of $27,343.21,23 One of the major reasons for the low annual income among Indigenous people stems from the history of residential schools, and the lack of formal educational opportunities which would confer vertical mobility to Indigenous peoples, allowing them to escape the poverty cycle.21 For over a century, the residential school system, operated by the federal government and religious institutions, forcibly removed Indigenous children from their families and communities.21 These schools often provided substandard education, with a stronger emphasis on manual labor, cultural assimilation, and discipline than on academic learning.5,21 As a result, many survivors were left without the literacy, credentials, or vocational training needed to access higher education or stable employment.21 The long-term effects of this systemic educational deprivation continue to hinder socioeconomic advancement for Indigenous peoples today.6,21 The cycle of poverty, in turn, exacerbates housing challenges, perpetuating the conditions that contribute to higher asthma prevalence in Indigenous communities.21,22
Cultural and Community-Based Impacts
Fenton et al. (2012) noted that a lack of culturally relevant materials for Indigenous families with children suffering from asthma.10 These included language-friendly pamphlets, brochures, and educational workshops.10 As such, one of the major barriers to care for asthmatic children in Indigenous communities is a lack of culturally competent care.24 The lack of culturally competent care is a significant concern, as it is associated with delays in seeking treatment, missed screenings, and increased feelings of alienation within the healthcare system.24 These factors contribute to poorer asthma outcomes for Indigenous children.24
Additionally, many Indigenous people, particularly those living in Northern communities, face significant access barriers to healthcare including shortage of primary care providers, ambulances, and medication.10,21 Fenton et al. reports that there is a lack of trained healthcare personnel that can provide adequate asthma care.10 It is critical to distinguish asthma from viral bronchiolitis in children, as the two conditions, while often presenting with similar respiratory symptoms such as wheezing and shortness of breath, require fundamentally different management approaches.25 Misdiagnosis can lead to inappropriate treatment—either the unnecessary use of bronchodilators in bronchiolitis or the failure to provide controller medications for asthma—which may worsen outcomes.25 This distinction is especially important in Indigenous communities, where limited access to pediatric specialists and diagnostic tools increases the likelihood of clinical uncertainty.10,21 Enhancing the availability of trained healthcare professionals in these regions is essential to ensure timely and accurate diagnoses and to reduce preventable respiratory complications in children.10,21
The logistical challenges of accessing medical care are particularly burdensome for Indigenous children with asthma.10 In some cases, Indigenous children living with asthma need a doctor’s note to bring puffers to school, yet the nearest doctor is 75-100 miles away.10 Moreover, even if a doctor’s note is acquired, lack of school-related asthma policies and training among teachers prevents them from administering puffers to children, even if they have asthmatic symptoms, leaving children solely responsible for managing their symptoms.10 As a result, without proper medication and management, a higher prevalence of poorly controlled asthma is noted in Indigenous compared to non-Indigenous children.10
Male vs. Female Differences
Research suggests that asthma prevalence varies by sex within Indigenous populations.9,11-17 Afzal (2022), Koleade et al. (2018), and Crighton et al. (2010), found that asthma prevalence was higher in Aboriginal women compared to men.9,14,17 Conversely, Crighton et al. (2010), Chang et al. (2012), Senthilselvan et al. (2015), and Karunanayake et al. (2020), found that asthma prevalence was higher in Indigenous boys compared to girls.11-13,17 Overall, there is some evidence that asthma prevalence can be stratified by sex as well as age.9,11-17
To understand these differences, it is important to examine sex- and age-specific risk factors.9,11,14,15,17 Indigenous women have higher rates of COPD, diabetes, and obesity as compared to men, and all three factors are associated with the development of asthma.26,27 Moreover, Koleade et al. (2018), found that the ACO was more common in Indigenous women compared to men. When understood in the context of other risk factors that affect both men and women, such as overcrowding, home dampness and low income, higher rates of comorbidities may explain why asthma prevalence is higher in Indigenous women compared to men.9,11-15,17
Interestingly, while some studies show that asthma prevalence is higher in Indigenous boys, girls have a higher prevalence of obesity and are more likely to smoke than boys.28.29 In contrast, Gao et al. (2008), found that Indigenous girls had a significantly higher prevalence of asthma compared to boys.16 As such, the relationship between sex and asthma risk in Indigenous youth remains unclear. One avenue of research that could reveal nuances in asthma prevalence is the ADAM33 mutation.30 ADAM33 has already been heavily implicated in asthma pathogenesis, so it is worth investigating whether single nucleotide polymorphisms in ADAM33, associated with increased asthma severity, are more common in Indigenous boys compared to girls.30 Genetic testing, if implemented, can help Indigenous families determine if their children are at risk of asthma, and take necessary therapeutic steps.30 Ultimately, examining the interplay between genetic and environmental risk factors can enhance our understanding of asthma development in Indigenous populations.9,11-17,30
Strengths and Limitations of the Present Review
This review stands out as the most recent and comprehensive synthesis of literature examining asthma in Indigenous populations in Canada. Unlike prior reviews that limited their searches to a single database, this study employed a rigorous methodology by sourcing articles from three major electronic databases—PubMed, Medline OVID, and EMBASE—thereby enhancing the breadth and inclusivity of the findings. Each of the 12 final articles was critically appraised for both strengths and limitations, providing readers with a transparent evaluation of the existing evidence. Moreover, this review offered several novel insights and forward-looking research directions that were not previously addressed in earlier reviews.
However, there are several limitations to this systematic review. There is a scarcity of literature surrounding asthma prevalence and risk factors among Canadian Indigenous populations, which limits the ability to draw definitive conclusions about asthma prevalence. Thus, the findings of this review may evolve as new research becomes available. Additionally, the search criteria employed may have inadvertently excluded relevant and insightful articles, particularly those focused on related respiratory diseases that could enrich our understanding.
Among the articles selected for inclusion, many obtained data from the same survey (APS), which made it challenging to critically evaluate differences among their results.11-13,17 The variability in study quality also presents challenges in synthesizing results across different contexts, potentially affecting the generalizability of the conclusions drawn.
Conclusion
This review highlights persistent disparities in asthma outcomes among Indigenous populations in Canada and underscores the need for targeted, culturally appropriate health policies. While national frameworks such as the NLHF have established important foundations for asthma care, they have yet to meaningfully integrate culturally competent, community-level interventions tailored to Indigenous populations. Broad, cross-sectoral collaboration—particularly involving Indigenous communities themselves—will be essential in developing effective solutions.
Improving asthma outcomes will require policies that are responsive to both the structural and cultural determinants of health. Investments in Indigenous-led health education, housing improvements, and equitable access to care are promising directions. Additionally, advancing this field will require more rigorous, community-based research that centers Indigenous voices and knowledge systems. Addressing these gaps through inclusive policy reform and high-quality evidence will be key to promoting health equity and reducing the burden of asthma in Indigenous communities.
Conflict of Interest Disclosure
There are no conflicts of interest to declare.
References
[1] Dharmage SC, Perret JL, Custovic A. Epidemiology of Asthma in Children and Adults. Front Pediatr. 2019 Jun 18;7. https://doi.org/10.3389/fped.2019.00246
[2] Radhakrishnan D, Guttmann A, To T, Reisman JJ, Knight BD, Mojaverian N, et al. Generational Patterns of Asthma Incidence among Immigrants to Canada over Two Decades. A Population-based Cohort Study. Ann Am Thorac Soc. 2019 Feb;16(2):248–57. https://doi.org/10.1513/AnnalsATS.201803-187OC
[3] Godbout K, Kim H, Mayers I, Paterson J, Chan CKN. A survey of severe asthma in Canada: results from the CASCADE practice reflective program. Allergy, Asthma & Clinical Immunology. 2024 Apr 18;20(1):31. https://doi.org/10.1186/s13223-024-00891-x
[4] Larsson K, Kankaanranta H, Janson C, Lehtimäki L, Ställberg B, Løkke A, et al. Bringing asthma care into the twenty-first century. NPJ Prim Care Respir Med. 2020 Jun 5;30(1):25. https://doi.org/10.1038/s41533-020-0182-2
[5] Sehgal A, Henderson R, Murry A, Crowshoe L, Barnabe C. Advancing health equity for Indigenous peoples in Canada: development of a patient complexity assessment framework. BMC Primary Care. 2024 Apr 29;25(1):144. https://doi.org/10.1186/s12875-024-02362-z
[6] Nguyen NH, Subhan FB, Williams K, Chan CB. Barriers and Mitigating Strategies to Healthcare Access in Indigenous Communities of Canada: A Narrative Review. Healthcare. 2020 Apr 26;8(2):112. https://doi.org/10.3390/healthcare8020112
[7] Sin DD, Wells H, Svenson LW, Man SFP. Asthma and COPD Among Aboriginals in Alberta, Canada. Chest. 2002 Jun;121(6):1841–6. https://doi.org/10.1378/chest.121.6.1841
[8] Kovesi T, Zaloum C, Stocco C, Fugler D, Dales R, Guay M, et al. Heat recovery ventilators prevent respiratory disorders in Inuit children. Indoor Air. 2009 Oct;19(5):489–99. doi:10.1111/j.1600-0668.2009.00606.x
[9] Afzal N. Asthma in First Nations Adults: Prevalence and Associated Factors. University of Saskatchewan; 2022.
[10] Fenton N, Latycheva O, Barker K, Gillespie JA, Elliott S, Vine M, et al. Assessing Needs: Asthma in First Nations and Inuit Communities in Canada. Pimatisiwin. 2012;10(1):71–81.
[11] Karunanayake CP, Amin K, Abonyi S, Dosman JA, Pahwa P. Prevalence and determinants of asthma among aboriginal adolescents in Canada. Journal of Asthma. 2020 Jan 2;57(1):40–6. https://doi.org/10.1080/02770903.2018.1541354
[12] Senthilselvan A, Niruban SJ, King M, Majaesic C, Veugelers P, Laing L, et al. Prevalence and risk factors of asthma in First Nations children living on reserves in Canada. Canadian Journal of Public Health. 2015 Nov 1;106(8):e483–8. https://doi.org/10.17269/CJPH.106.5147
[13] Chang HJ, Beach J, Senthilselvan A. Prevalence of and Risk Factors for Asthma in Off-Reserve Aboriginal Children and Adults in Canada. Can Respir J. 2012;19(6):e68–74. https://doi.org/10.1155/2012/753040
[14] Koleade A, Farrell J, Mugford G, Gao Z. Prevalence and Risk Factors of ACO (Asthma-COPD Overlap) in Aboriginal People. J Environ Public Health. 2018 Nov 21;2018:1–9. https://doi.org/10.1155/2018/4657420
[15] Koleade A, Farrell J, Mugford G, Gao Z. Female-specific risk factors associated with risk of ACO (asthma COPD overlap) in aboriginal people. Journal of Asthma. 2020 Sep 1;57(9):925–32. https://doi.org/10.1080/02770903.2019.1621890
[16] Gao Z, Rowe BH, Majaesic C, O’Hara C, Senthilselvan A. Prevalence of Asthma and Risk Factors for Asthma‐Like Symptoms in Aboriginal and Non‐Aboriginal Children in the Northern Territories of Canada. Can Respir J. 2008 Jan;15(3):139–45. https://doi.org/10.1155/2008/302407
[17] Crighton EJ, Wilson K, Senècal S. The relationship between socio-economic and geographic factors and asthma among Canada’s Aboriginal populations. Int J Circumpolar Health. 2010 Apr 26;69(2):138–50. https://doi.org/10.3402/ijch.v69i2.17435
[18] Riva M, Fletcher C, Dufresne P, Lanari M, Potvin L, Perreault K, et al. Relocating to a new or pre-existing social housing unit: significant health improvements for Inuit adults in Nunavik and Nunavut. Can J Public Health. 2020 Feb;111(1):21–30. 10.17269/s41997-019-00249-6
[19] Lyeo JS, Wong MD, Clyke N, Canoe BB, Kinnear P, Stopps H, et al. Ten questions concerning First Nations on-reserve housing in Canada. Build Environ. 2024 Jun;257:111544. https://doi.org/10.1016/j.buildenv.2024.111544
[20] Webster PC. Housing triggers health problems for Canada’s First Nations. The Lancet. 2015 Feb;385(9967):495–6. https://doi.org/10.1016/s0140-6736(15)60187-8
[21] Richmond CAM, Cook C. Creating conditions for Canadian aboriginal health equity: the promise of healthy public policy. Public Health Rev. 2016 Dec 20;37(1):2. https://doi.org/10.1186/s40985-016-0016-5
[22] Hajizadeh M, Hu M, Bombay A, Asada Y. Socioeconomic inequalities in health among Indigenous peoples living off-reserve in Canada: Trends and determinants. Health Policy (New York). 2018 Aug;122(8):854–65. https://doi.org/10.1016/j.healthpol.2018.06.011
[23] Statistics Canada. Quality of life indicator: Poverty. Available from: https://www160.statcan.gc.ca/prosperity-prosperite/poverty-pauvrete-eng.htm
[24] O’Sullivan B. Considering culture in Aboriginal care. Can Med Assoc J. 2013 Jan 8;185(1):E27–8. https://doi.org/10.1503/cmaj.109-4376
[25] Kovesi T, Giles B, Pasterkamp H. Long-term management of asthma in First Nations and Inuit children: A knowledge translation tool based on Canadian paediatric asthma guidelines, intended for use by front-line health care professionals working in isolated communities. Paediatr Child Health. 2012 Aug 1;17(7):e46–64. https://doi.org/10.1093/pch/17.7.e46
[26] Bird Y, Moraros J, Mahmood R, Esmaeelzadeh S, Kyaw Soe NM. Prevalence and associated factors of COPD among Aboriginal peoples in Canada: a cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2017 Jun;Volume 12:1915–22. https://doi.org/10.2147/COPD.S138304
[27] Batal M, Decelles S. A Scoping Review of Obesity among Indigenous Peoples in Canada. J Obes. 2019 Jun 3;2019:1–20. https://doi.org/10.1155/2019/9741090
[28] Elton-Marshall T, Leatherdale ST, Burkhalter R. Tobacco, alcohol and illicit drug use among Aboriginal youth living off-reserve: results from the Youth Smoking Survey. Can Med Assoc J. 2011 May 17;183(8):E480–6. https://doi.org/10.1503/cmaj.101913
[29] Kolahdooz F, Sadeghirad B, Corriveau A, Sharma S. Prevalence of overweight and obesity among indigenous populations in Canada: A systematic review and meta-analysis. Crit Rev Food Sci Nutr. 2017 May 3;57(7):1316–27. https://doi.org/10.1080/10408398.2014.913003
[30] Sleziak J, Gawor A, Błażejewska M, Antosz K, Gomułka K. ADAM33′s Role in Asthma Pathogenesis: An Overview. Int J Mol Sci. 2024 Feb 15;25(4):2318. https://doi.org/10.3390/ijms25042318
[31] Marciniuk D. The national lung health framework – “what we have been asking for….” Can Respir J. 2007 Apr;14(3):139–40.
[32] Chapman A. THE NATIONAL LUNG HEALTH FRAMEWORK (CANADA). Chest. 2008 Oct;134(4):115P. https://doi.org/10.1378/chest.134.4_MeetingAbstracts.p115001