UOJM AHEAD OF PRINT
RESEARCH
Temporal Trends in Mental Health Terminology in Skin Cancer Clinical Trials from the ClinicalTrials.gov Database
2 Faculty of Applied Science and Engineering, University of Toronto, Toronto, ON, Canada
3 Department of Psychiatry, Faculty of Medicine, University of Ottawa, Ottawa, ON, Canada
4 Mental Health Department, Queensway Carleton Hospital, Nepean, ON, Canada
University of Ottawa Journal of Medicine, Ahead of Print, June 2026,
https://doi.org/10.18192/UOJM.V16i1.7898
Keywords: Anxiety, Depression, Stress, Distress, Mental Health, Skin Neoplasms, Oncology, Clinical Trials.
Abstract
Objective: This study aims to assess temporal trends in
the inclusion of mental health (MH)-related terminology in skin cancer
(SC) clinical trials as a proxy for research interest, and to evaluate
whether the COVID-19 pandemic influenced the appearance of such terms.
Methods: This retrospective descriptive analysis
extracted 6,063 SC clinical trials from the U.S. National Library of
Medicine’s ClinicalTrials.gov database, dating back to 1976. The annual
count and frequency of the terms “anxiety”, “stress”, “distress”, and
“depression” were tabulated using a Python program.
Results: The year of study initiation was significantly
positively associated with the appearance of these MH terms, while the
COVID-19 pandemic had no significant impact. The analysis was limited to
terminology on ClinicalTrials.gov and may not fully capture the extent
of MH considerations in study design or outcomes.
Conclusion: These findings suggest a small, yet
growing, emphasis on MH in SC clinical trials.
Résumé
Objectif : Cette étude vise à évaluer les tendances
temporelles concernant l’inclusion de termes liés à la santé mentale
(SM) dans les essais cliniques sur le cancer de la peau (CP), en tant
qu’indicateur de l’intérêt de la recherche, et à déterminer si la
pandémie de COVID-19 a influencé l’apparition de ces termes.
Méthodes : Cette analyse descriptive rétrospective a
extrait 6,063 essais cliniques sur le CP de la base de données
ClinicalTrials.gov de la Bibliothèque nationale de médecine des
États-Unis, remontant jusqu’à 1976. Le nombre annuel et la fréquence des
termes « anxiety », « stress », « distress » et « depression » ont été
tabulés à l’aide d’un programme Python.
Résultats :
L’année de lancement de l’étude était significativement et positivement
associée à l’apparition de ces termes liés à la SM, tandis que la
pandémie de COVID-19 n’a pas eu d’impact significatif. L’analyse était
limitée à la terminologie présente sur ClinicalTrials.gov et pourrait ne
pas refléter pleinement l’ampleur des considérations accordées à la SM
dans la conception des études ou leurs résultats.
Conclusion
: Ces résultats suggèrent une importance modeste, mais
croissante, sur la SM dans les essais cliniques sur le CP.
Introduction
Background
Skin cancer (SC) is an overarching term that encompasses all forms of cancer of the skin including basal cell carcinoma, squamous cell carcinoma, and melanoma.1 SC remains the most commonly diagnosed cancer worldwide, with over 1.5 million new cases in 2022.2,3 This underscores the growing need for a comprehensive understanding of all aspects of this disease, including the mental toll it takes on those affected.
Mental health (MH) conditions, such as depression, anxiety, stress, and distress, have been associated with SC.4–8 A cross-sectional study examining the association between MH conditions and SC found that individuals with MH disorders had significantly greater odds of developing SC.8 Furthermore, although discussions about social and emotional needs are associated with a 55% reduction in the odds of depressive symptoms, only 33.6% of SC survivors are estimated to have had such conversations.9
The terms “anxiety”, “stress”, “distress”, and “depression” have been particularly associated with SC in the literature. For “distress”, one study found that 19% of non-melanoma SC patients experience significant psychological distress, with those who coped by avoidance being more susceptible.10 Psychological distress has been shown to reduce treatment adherence, delay medical help-seeking, and lower engagement in post-treatment preventative behaviors and SC screening.4,8 More aggressive SCs like melanoma may be particularly psychologically impactful, likely due to the life-threatening nature of the disease.5 For “stress”, cancer treatment can be extensive, drastically altering one’s life and causing profound stress and uncertainty.11 For “depression”, over 10% of all cancer patients are depressed, likely due to the considerable psychological and emotional burden inherent in such a diagnosis.12 Kungwengwe et al. found that 18.4% of cutaneous malignant melanoma patients experience depression, with peak incidence during treatment.13 “Anxiety” has also been linked to SC, demonstrating a prevalence of 30.6% in SC patients.13 Advanced-stage melanoma patients were also found to score higher on the phobic anxiety scale than those in the initial stages, demonstrating a correlation between MH symptoms and SC severity.14
Rationale and Objectives
Over the past few decades, particularly since 2010, research on MH has steadily increased.15 Whether this trend is reflected in the context of SC research remains unclear. The objective of this study is to capture the frequency of MH terms in SC clinical trial summaries over time as a proxy measure for research interest. From our review of the literature, this study is the first to examine MH in SC clinical trials as a metric for research interest in mental illness. Previous research explored a similar methodology in Alzheimer’s disease.16 This was subsequently reproduced in two studies concerning erectile dysfunction and multiple sclerosis.17,18 SC was a natural avenue to further explore our extraction program due to its strong association with MH.7,8
Golrokhian-Sani et al.’s pilot study found an increase in MH terminology over time and following the COVID-19 pandemic.16 We therefore hypothesize a similar trend: an increase in the frequency of MH terminology in SC clinical trials over time.
Methods
Study Design
In January 2024, all clinical trials associated with the keyword “Skin Cancer” and with a start date between 1976 and 2023 were extracted from the U.S. National Library of Medicine's ClinicalTrials.gov database (Supplemental Figure 1). ClinicalTrials.gov was chosen for its international scope and extensive records, which would strengthen the generalizability of this study. No patient medical files were accessed; therefore, no consent was required. Extracted data included the National Clinical Trial number, start date, and a JavaScript Object Notation file with more detailed information about each study. Only trials with a “completed” status were included.
We adapted a Python program from the Golrokhian-Sani et al. paper to process each trial’s brief description.16 The brief description represents a concise summary of the work, so if an MH condition was truly assessed in a trial, it would likely be mentioned there. It was chosen based on the Python code adapted from the pilot study. This Python program filtered the descriptions by splitting the text into a list of words and replacing instances of punctuation, dashes, numbers, and apostrophes with whitespace. Apostrophes followed by an “s” (i.e., ‘s) at the end of any word were removed. All text was converted to lowercase. Other than the aforementioned modifications, the program only extracted exact matches. It did not account for plural terms or related variations. For instance, if a paper mentioned the term “stressors” instead of “stress”, it would not be counted as an MH term.
Outcome
The Python program counted the frequency of four MH-related terms associated with SC: “depression”, “anxiety”, “distress”, and “stress”.4,5,7,8 Although other MH-related terms appear in the literature, these four are among the most consistently associated with SC. In this study, the frequency of these terms in the brief descriptions serves as a proxy for research interest. Frequency was defined as the number of trials in which an MH term appeared in the brief description section. A term was counted once per study, regardless of how many times it appears (i.e., binary yes/no).
Statistical Analysis
Binary logistic regression analyses were conducted in SPSS 29.0.2.0 to assess the relationship between the year of start date and the MH term mentioned in SC registered trials.19 The dependent variable was a categorical (yes/no) value to indicate whether a registered trial in a given year mentioned an MH term, with the independent variable being the trial start year. Analyses were conducted separately for each term. Binary logistic regressions were also conducted to assess the impact of the COVID-19 pandemic on the presence of MH terms. The year 2020 was used as a cutoff: studies from 2016-2019 were coded as “pre-COVID” and studies from 2020-2023 were coded as “post-COVID”. Studies prior to 2016 were excluded to minimize the confounding effects of increasing public awareness of MH over time. A multicollinearity analysis was performed to assess potential interactions among the MH term mentions, the trial start year, and whether the study was conducted during the COVID-19 period. This was conducted to ensure that the relationship between MH term mentions and the COVID-19 period was not mediated by MH term mentions over time (i.e., trial start year). Analyses were two-sided, and p-values < 0.05 were considered statistically significant. The regression coefficient (B) was used to assess the strength of the association.
Results
A total of 6,063 studies were included. The overall volume of studies increased over time (Figure 1). However, a noticeable decrease in the number of completed studies was observed beginning in 2020.
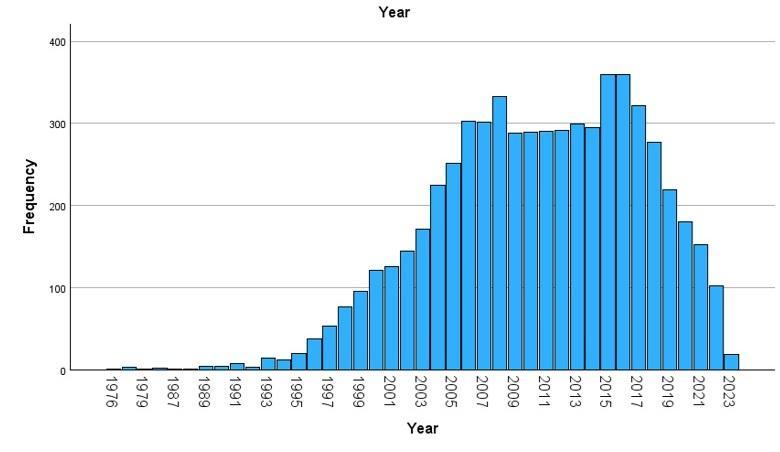
Figure 1. Volume of completed studies over time. The x-axis indicates the trial start year and the y-axis indicates the number of completed studies within a given trial start year.
Results of the logistic regression for the association between study start year and the mention of MH terms in a given year are presented in Table 1. A statistically significant positive association was observed between the study start year and the presence of each of the four MH terms: “depression,” “anxiety,” “stress,” and “distress.” However, the magnitude of these relationships, as indicated by B, was small (i.e. <0.2).
Table 1. Binary logistic regression analysis of the association between start year and mention of MH terms (n=6,063).
| MH term | ß | Standard Error | P-value | Exp(ß) | Lower 95% CI for Exp(ß) | Upper 95% CI for Exp(ß) | Log likelihood | Wald score |
|---|---|---|---|---|---|---|---|---|
| Depression | .107 | .020 | <.001 | 1.113 | 1.071 | 1.156 | -450.90 | 29.901 |
| Anxiety | .145 | .018 | <.001 | 1.156 | 1.115 | 1.198 | -558.28 | 62.497 |
| Stress | .046 | .015 | .002 | 1.047 | 1.017 | 1.078 | -603.76 | 9.782 |
| Distress | .075 | .016 | <.001 | 1.078 | 1.044 | 1.112 | -558.13 | 21.382 |
| MH: Mental health | ||||||||
No significant association was found between the COVID-19 period and the presence of MH terms (Table 2). The multicollinearity analysis variance inflation factors were one for all four MH terms, indicating no collinearity.
Table 2. Binary logistic regression analysis of the impact of COVID-19 on MH terms, 2016-2023 (n=1,630).
| MH term | ß | Standard Error | P-value | Exp(ß) | Lower 95% CI for Exp(ß) | Upper 95% CI for Exp(ß) | Log likelihood | Wald score |
|---|---|---|---|---|---|---|---|---|
| Depression | .100 | .324 | .757 | 1.106 | .586 | 2.086 | -963.24 | 0.261 |
| Anxiety | .466 | .250 | .062 | 1.594 | .977 | 2.602 | -961.615 | 5.597 |
| Stress | -.533 | .396 | .178 | .587 | .270 | 1.274 | -962.28 | 0.096 |
| Distress | -.421 | .343 | .219 | .656 | .335 | 1.284 | -962.47 | 4.138 |
| MH: Mental health | ||||||||
Figure 2 and Table 3 illustrate the trajectory of the proportion of studies mentioning MH terms over time based on data from 1976 to 2023 (Maximum probability = 1). The data fit exponential models, with R2 = 1 for all MH terms.
Table 3. Trajectory of MH term mentions over time.
| MH term | Mathematical trajectory | Predicted probability of MH term mention in 2040 (%) |
|---|---|---|
| Distress | y = 1E-66*e^(0.0735*x) | 0.131 (13.1) |
| Stress | y = 8E-42*e^(0.0451*x) | 0.072 (7.2) |
| Anxiety | y = 3E-127*e^(0.1427*x) | 0.801 (80.1) |
| Depression | y = 1E-94*e^(0.1054*x) | 0.240 (24.0) |
| MH: Mental health, y: predicted probability of MH mention, x: year | ||
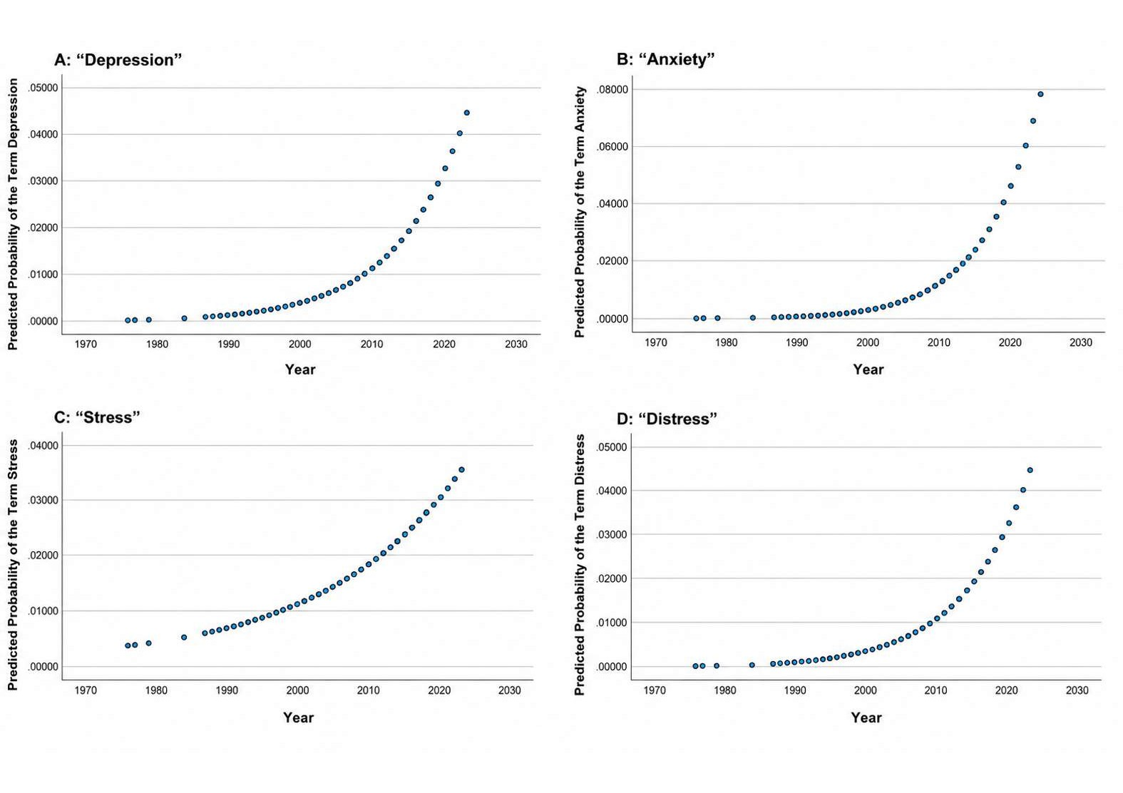
Figure 2. Predicted probabilities of MH term mentions over time. The x-axis indicates the trial start year and the y-axis indicates the probability of an MH mention with maximum probability = 1. Trajectories were modelled exponentially with R2 = 1 for all MH terms. The model for (A) “depression” was y = 1E-94*e^(0.1054*x). The model for (B) “anxiety” was y = 3E-127*e^(0.1427*x). The model for (C) “stress” was y = 8E-42*e^(0.0451*x). The model for (D) “distress” was y = 1E-66*e^(0.0735*x).
Discussion
The results of the binary logistic regression analysis between the study start year and the presence of MH terminology (Table 1) suggest an increased acknowledgment of MH in SC clinical trials. Mentions of “depression”, “anxiety”, “stress”, and “distress” have all significantly increased over time. Despite MH terminology presence acting only as a proxy for true research interest, this trend may reflect a growing awareness of MH, fueled by greater understanding and visibility of MH conditions. There have been measurable improvements in MH literacy over time, with the public more open to psychotherapy and pharmacological treatments for MH disorders, potentially leading to similar trends in research.20,21 Another study reported a modest rise in psychological distress and a more substantial increase in treatment-seeking over the past two decades.22 Regardless of which factor predominates, they ultimately suggest that MH is receiving greater attention in the clinical and research spheres. Despite the increase in MH terminology in SC research, the magnitude of these associations over time remains small (Table 1). This suggests that while MH may be gaining visibility, it may not yet be a primary focus in the majority of SC clinical trials. This is particularly interesting, given the documented impact of SC on MH and quality of life in affected individuals.10,12 Failing to address MH psychological symptoms in SC populations may contribute to suboptimal therapeutic outcomes.23,24
We also conducted an analysis to project the prevalence of MH terms mentioned in SC trials over time (Figure 2, Table 3). With this fixed model, all four terms are expected to increase, with “anxiety” showing the steepest projected growth. However, these projections likely overestimate future trends, as they are based on recent exponential growth that may naturally plateau over time and do not account for shifting clinical priorities. These projections should thus be interpreted cautiously.
There was no significant change in the mention of MH terminology in SC research before and after the onset of the COVID-19 pandemic (Table 2), despite its widespread impact on MH globally.25 Several factors related to the logistics of conducting clinical trials during the pandemic may explain this finding. Studies faced numerous challenges, including personnel shortages, difficulties with follow-up, and limited access to medical facilities.26,27 Isolation protocols and financial constraints likely made recruitment difficult. With healthcare budgets stretched thin, studies investigating both SC and MH may have been deprioritized.28 Additionally, because clinical trials require significant time to plan and implement, many studies launched or completed after 2020 may still reflect pre-pandemic priorities. This may have led to a significant interpretive limitation, considering the post-COVID era may have been comparatively underrepresented. As Morris et al. note, it often takes years for research practices to adapt to new developments.29 Notably, studies prior to 2016 were excluded from this analysis, reducing the effect of this limitation.
Implications
MH is an essential element of holistic management, and its growing presence in SC research is a promising sign. However, this paper highlights the need to further incorporate MH into SC research. Future clinical trials should include MH screening tools, research should be conducted to guide clinicians toward more integrated models of care, and routine psychological screening may allow for earlier identification of MH concerns. Preventive approaches, such as facilitating appropriate referrals, can enhance patient quality of life and treatment outcomes.24,30
Limitations
There are limitations inherent to this study. We did not extract the context in which MH terms were used; instead, we treated any appearance of a term as an indication that researchers intended to address that MH condition. As such, term frequency does not necessarily reflect the depth or quality of discussion. On the other hand, the absence of MH terms may not necessarily indicate the absence of its assessment through other methods (e.g., psychological assessments, quality-of-life questionnaires, patient-reported measures). Thus, future studies should aim to capture contextual information, such as whether MH terms appear in the objective statement or experimental protocol, to better assess research focus.18 Additionally, we only extracted terms from the brief description section of each clinical trial. If an MH term appeared elsewhere, it would not have been captured in our analysis. Expanding this methodology to include additional sections may allow for a more comprehensive understanding of MH representation. In the same vein, the selection of the MH terms may have produced different representations of research interest: depression, for example, is a long-studied topic, with many articles reporting a continuous increase in its prevalence.31,32 It may have also artificially led to a reduced number of MH term appearances, as oncology often measures MH through broader frameworks (e.g., quality of life). Finally, the Python program used only extracted exact key term matches, potentially leading to an underrepresentation of MH conditions. To help mitigate this, the program deleted any punctuation, dashes, numbers, and apostrophes.
Conclusion
In this study, we analyzed the presence of MH terms (“depression”, “anxiety”, “stress”, and “distress”) in SC clinical trial summaries. A statistically significant association was found between the study start year and the mention of each MH term, suggesting a small yet growing recognition of MH in SC research. No significant change was observed based on COVID-19 status. Future studies that extract the full context of MH terms may help identify more specific trends.
Conflicts of Interest Disclosure
There are no conflicts of interest to declare.
Data Availability
The Python code and the exported data can be accessed at: https://zenodo.org/records/14722603
References
Linares MA, Zakaria A, Nizran P. Skin Cancer. Prim Care Clin Off Pract. 2015 Dec;42(4):645–59. doi:10.1016/j.pop.2015.07.006
International Agency for Research on Cancer. IARC [Internet]. 2024. Skin cancer. Available from: https://www.iarc.who.int/cancer-type/skin-cancer/
US Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent Skin Cancer. [Internet]. Washington (DC): Office of the Surgeon General; 2014. Available from: https://www.ncbi.nlm.nih.gov/books/NBK247164/
Gogas HJ, Karalexi MA, Dessypris N, Antoniadis AG, Papadopoulos F, Petridou ET. The role of depression and personality traits in patients with melanoma: a South-European study. Melanoma Res. 2017 Dec;27(6):625–31. doi:10.1097/CMR.0000000000000380
Kasparian NA, McLoone JK, Butow PN. Psychological Responses and Coping Strategies Among Patients With Malignant Melanoma: A Systematic Review of the Literature. Arch Dermatol. 2009 Dec 1;145(12). doi:10.1001/archdermatol.2009.308
National Cancer Institute. National Cancer Institute [Internet]. 2024. Cancer-Related Post-Traumatic Stress (PDQ®)–Patient Version. Available from: https://www.cancer.gov/about-cancer/coping/survivorship/new-normal/ptsd-pdq
Radiotis G, Roberts N, Czajkowska Z, Khanna M, Körner A. Nonmelanoma Skin Cancer: Disease-Specific Quality-of-Life Concerns and Distress. Oncol Nurs Forum. 2014 Jan 1;41(1):57–65. doi:10.1188/14.ONF.57-65
Tkachenko E, Singer S, Mostaghimi A, Hartman RI. Association of poor mental health and skin cancer development: a cross-sectional study of adults in the United States. Eur J Cancer Prev. 2020 Nov;29(6):520–2. doi:10.1097/CEJ.0000000000000567
Hong YR, Yadav S, Suk R, Khanijahani A, Erim D, Turner K. Patient-provider discussion about emotional and social needs, mental health outcomes, and benefit finding among U.S. Adults living with cancer. Cancer Med. 2021 Jun;10(11):3622–34. doi:10.1002/cam4.3918
Roberts N, Czajkowska Z, Radiotis G, Körner A. Distress and Coping Strategies Among Patients with Skin Cancer. J Clin Psychol Med Settings. 2013 Jun;20(2):209–14. doi:10.1007/s10880-012-9319-y>
Hulin C, Hansen T, Heron L, Pughe R, Streetly M, Plate A, et al. Living with the burden of relapse in multiple myeloma from the patient and physician perspective. Leuk Res. 2017 Aug;59:75–84. doi:10.1016/j.leukres.2017.05.019
Smith HR. Depression in cancer patients: Pathogenesis, implications and treatment (Review). Oncol Lett. 2015 Apr;9(4):1509–14. doi:10.3892/ol.2015.2944
Kungwengwe G, Gowthorpe C, Ali SR, Warren H, Drury DJ, Ang KL, et al. Prevalence and odds of anxiety and depression in cutaneous malignant melanoma: a proportional meta-analysis and regression. Br J Dermatol. 2024 Jun 20;191(1):24–35. doi:10.1093/bjd/ljae011
Kontoangelos K, Nikolaou V, Syrgianni A, Tsiori S, Papageorgiou C, Stratigos A. Correlation of Psychosomatic Factors and Personality Traits With the Severity of Melanoma. Vivo Athens Greece. 2024;38(6):2844–52. doi:10.21873/invivo.13765
Hernández-Torrano D, Ibrayeva L, Sparks J, Lim N, Clementi A, Almukhambetova A, et al. Mental Health and Well-Being of University Students: A Bibliometric Mapping of the Literature. Front Psychol. 2020 Jun 9;11:1226. doi:10.3389/fpsyg.2020.01226
Golrokhian-Sani AA, Morcos M, Philippi A, Al-Rawi R, Morcos M, Rui F. Temporal Trends in Mental Health Terminology in Alzheimer’s Disease Clinical Trials. PLOS ONE. Forthcoming. 2024;19(12):e0310264. doi:10.1371/journal.pone.0310264
Morcos M, Jeryous Fares B, Golrokhian-Sani AA, Morcos M, Flannigan R, Breau RH, et al. Prevalence of mental health evaluation in erectile dysfunction clinical trials. J Sex Med. 2025 Jul 23;22(9):1665-72. doi:10.1093/jsxmed/qdaf173
Phillips B, Singh H, Morcos M, Golrokhian-Sani AA, Morcos M, Fu R. Trends in Neuropsychiatric Terminology Use Within Registered Clinical Trials for Multiple Sclerosis: A Retrospective Descriptive Analysis. Healthcare. 2025 Jan;13(20):2593. doi:10.3390/healthcare13202593
IBM SPSS Statistics for Windows. Version 29.0.2.0. IBM Corp; 2024.
Schomerus G, Schwahn C, Holzinger A, Corrigan PW, Grabe HJ, Carta MG, et al. Evolution of public attitudes about mental illness: a systematic review and meta-analysis: Evolution of public attitudes. Acta Psychiatr Scand. 2012 Jun;125(6):440–52. doi:10.1111/j.1600-0447.2012.01826.x
Angermeyer MC, Matschinger H, Schomerus G. Attitudes towards psychiatric treatment and people with mental illness: changes over two decades. Br J Psychiatry. 2013 Aug;203(2):146–51. doi:10.1192/bjp.bp.112.122978
Johnson AL. Changes in Mental Health and Treatment, 1997–2017. J Health Soc Behav. 2021 Mar;62(1):53–68. doi:10.1177/0022146520984136
Colucci R, Moretti S. The role of stress and beta-adrenergic system in melanoma: current knowledge and possible therapeutic options. J Cancer Res Clin Oncol. 2016 May;142(5):1021–9. doi:10.1007/s00432-015-2078-z
Sanzo M, Colucci R, Arunachalam M, Berti S, Moretti S. Stress as a Possible Mechanism in Melanoma Progression. Davids LM, editor. Dermatol Res Pract. 2010 Jan;2010(1):483493. doi:10.1155/2010/483493
Cullen W, Gulati G, Kelly BD. Mental health in the COVID-19 pandemic. QJM Int J Med. 2020 May 1;113(5):311–2. doi:10.1093/qjmed/hcaa110
Sathian B, Asim M, Banerjee I, Pizarro AB, Roy B, van Teijlingen ER, et al. Impact of COVID-19 on clinical trials and clinical research: A systematic review. Nepal J Epidemiol. 2020 Sep;10(3):878–87. doi:10.3126/nje.v10i3.31622
AlNaamani K, AlSinani S, Barkun AN. Medical research during the COVID-19 pandemic. World J Clin Cases. 2020 Aug 6;8(15):3156–63. doi:10.12998/wjcc.v8.i15.3156
Wager E, McGough M, Rakshit S, Cox C. How does health spending in the U.S. compare to other countries? [Internet]. Peterson-KFF; 2026 Mar. (Health Spending). Available from: https://www.healthsystemtracker.org/chart-collection/health-spending-u-s-compare-countries/#Health%20expenditures%20as%20percent%20of%20GDP,%201970-2023
Morris ZS, Wooding S, Grant J. The answer is 17 years, what is the question: understanding time lags in translational research. J R Soc Med. 2011 Dec;104(12):510–20. doi:10.1258/jrsm.2011.110180
Bhakta S, Brambert L, Bartlett G, Palnati SR, Mynam RS. Exploring the Psychological Experiences of Patients With Melanoma: A Narrative Review. Cureus. 2025 Feb 25;17(2):e79637. doi:10.7759/cureus.79637
Andersen I, Thielen K, Bech P, Nygaard E, Diderichsen F. Increasing prevalence of depression from 2000 to 2006. Scand J Public Health. 2011 Dec;39(8):857–63. doi:10.1177/1403494811424611
Klerman GL. Increasing Rates of Depression. JAMA J Am Med Assoc. 1989 Apr 21;261(15):2229. doi:10.1001/jama.1989.03420150079041